What Exactly Is Calcaneal Apophysitis?
Overview
Sever's disease is a painful irritation in the heel bone of the foot. It is the most common cause of heel pain in children and teens. Sever?s disease is also called calcaneal apophysitis.
Causes
This condition most commonly occurs due to repetitive or prolonged activities placing strain on the heel's growth plate, typically during a period of rapid growth. These activities (or sports) usually involve excessive walking, running, jumping or hopping. Severs disease may also be more likely to occur following a poorly rehabilitated sprained ankle, in patients with poor foot biomechanics or those who use inappropriate footwear. In young athletes, this condition is commonly seen in running and jumping sports, such as football, basketball, netball and athletics.
Symptoms
Children aged between 8 to 13 years of age can experience Sever?s disease with girls being normally younger and boys slightly older. Sever?s disease normally involves the back of the heel bone becoming painful towards the end of intense or prolonged activity and can remain painful after the activity for a few hours. Severe cases can result in limping and pain that can even remain the next morning after sport.
Diagnosis
In Sever's disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she runs or jumps. He or she may have a tendency to tiptoe. Your child's heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your doctor may also find that your child's heel tendons have become tight.
Non Surgical Treatment
The physiotherapist will thoroughly assess the affected areas and general mechanics to determine what factors may be contributing, also to rule out any other injuries or stress fractures, etc. Treatment focusing on the affected area will consist of modified rest, ice, massage, stretches and electrotherapy. A foam heel raise may also be given to help decrease pain. The physiotherapist may also treat other areas if biomechanical problems are noted. This may include massage, mobilization and exercises to stretch and strengthen certain areas. They may also refer the patient to see a podiatrist if they believe the foot posture is a factor.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever's disease is a painful irritation in the heel bone of the foot. It is the most common cause of heel pain in children and teens. Sever?s disease is also called calcaneal apophysitis.
Causes
This condition most commonly occurs due to repetitive or prolonged activities placing strain on the heel's growth plate, typically during a period of rapid growth. These activities (or sports) usually involve excessive walking, running, jumping or hopping. Severs disease may also be more likely to occur following a poorly rehabilitated sprained ankle, in patients with poor foot biomechanics or those who use inappropriate footwear. In young athletes, this condition is commonly seen in running and jumping sports, such as football, basketball, netball and athletics.
Symptoms
Children aged between 8 to 13 years of age can experience Sever?s disease with girls being normally younger and boys slightly older. Sever?s disease normally involves the back of the heel bone becoming painful towards the end of intense or prolonged activity and can remain painful after the activity for a few hours. Severe cases can result in limping and pain that can even remain the next morning after sport.
Diagnosis
In Sever's disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she runs or jumps. He or she may have a tendency to tiptoe. Your child's heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your doctor may also find that your child's heel tendons have become tight.
Non Surgical Treatment
The physiotherapist will thoroughly assess the affected areas and general mechanics to determine what factors may be contributing, also to rule out any other injuries or stress fractures, etc. Treatment focusing on the affected area will consist of modified rest, ice, massage, stretches and electrotherapy. A foam heel raise may also be given to help decrease pain. The physiotherapist may also treat other areas if biomechanical problems are noted. This may include massage, mobilization and exercises to stretch and strengthen certain areas. They may also refer the patient to see a podiatrist if they believe the foot posture is a factor.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Does Adult Aquired Flat Feet Always Require Surgery Teatment ?
Overview
Posterior tibial tendon dysfunction is one of several terms to describe a painful, progressive flatfoot deformity in adults. Other terms include posterior tibial tendon insufficiency and adult acquired flatfoot. The term adult acquired flatfoot is more appropriate because it allows a broader recognition of causative factors, not only limited to the posterior tibial tendon, an event where the posterior tibial tendon looses strength and function. The adult acquired flatfoot is a progressive, symptomatic (painful) deformity resulting from gradual stretch (attenuation) of the tibialis posterior tendon as well as the ligaments that support the arch of the foot. 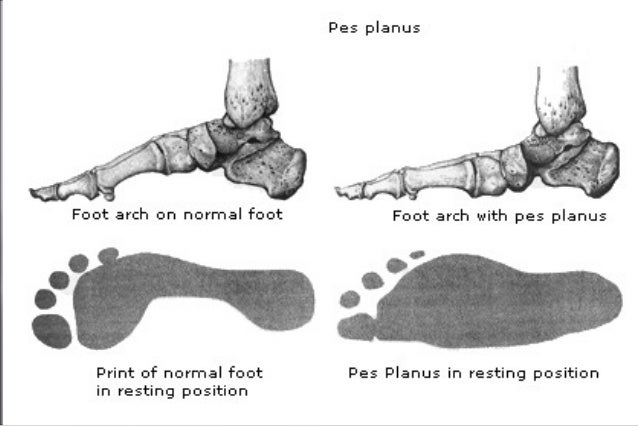
Causes
As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
Pain and swelling around the inside aspect of the ankle initially. Later, the arch of the foot may fall (foot becomes flat), this change leads to walking to become difficult and painful, as well as standing for long periods. As the flat foot becomes established, pain may progress to the outer part of the ankle. Eventually, arthritis may develop.
Diagnosis
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable. The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise. A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet - the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non surgical Treatment
Icing and anti-inflammatory medications can reduce inflammation and physical therapy can strengthen the tibial tendon. Orthotic inserts that go inside your shoes are a common way to treat and prevent flatfoot pain. Orthotics control the position of the foot and alleviate areas of pressure. In some cases immobilization in a cast or walking boot is necessary to relieve symptoms, and in severe cases surgery may be required to repair tendon damage. 
Surgical Treatment
Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Flat Feet In Adults
Overview
Adult acquired flatfoot deformity (AAFD) is a painful condition resulting from the collapse of the longitudinal (lengthwise) arch of the foot. As the name suggests, this condition is not present at birth or during childhood. It occurs after the skeleton is fully matured. In the past it was referred to a posterior tibial tendon dysfunction (or insufficiency). But the name was changed because the condition really describes a wide range of flatfoot deformities. AAFD is most often seen in women between the ages of 40 and 60. This guide will help you understand how the problem develops, how doctors diagnose the condition, what treatment options are available.
Causes
Damage to the posterior tendon from overuse is the most common cause for adult acquired flatfoot. Running, walking, hiking, and climbing stairs are activities that add stress to this tendon, and this overuse can lead to damage. Obesity, previous ankle surgery or trauma, diabetes (Charcot foot), and rheumatoid arthritis are other common risk factors.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle. Symptoms, which may occur in some persons with flexible flatfoot, include. Pain in the heel, arch, ankle, or along the outside of the foot. ?Turned-in? ankle. Pain associated with a shin splint. General weakness / fatigue in the foot or leg.
Diagnosis
There are four stages of adult-acquired flatfoot deformity (AAFD). The severity of the deformity determines your stage. For example, Stage I means there is a flatfoot position but without deformity. Pain and swelling from tendinitis is common in this stage. Stage II there is a change in the foot alignment. This means a deformity is starting to develop. The physician can still move the bones back into place manually (passively). Stage III adult-acquired flatfoot deformity (AAFD) tells us there is a fixed deformity. This means the ankle is stiff or rigid and doesn???t move beyond a neutral (midline) position. Stage IV is characterized by deformity in the foot and the ankle. The deformity may be flexible or fixed. The joints often show signs of degenerative joint disease (arthritis).
Non surgical Treatment
Initial treatment consists of supporting the medial longitudinal arch (running the length of the foot) to relieve strain on the medial soft tissues. The most effective way to relieve pain on the tendon is to use a boot or brace, and once tenderness and pain has resolved, an orthotic device. A boot, brace, or orthotic has not been shown to correct or even prevent the progression of deformity. Orthotics can alleviate symptoms and may slow the progression of deformity, particularly if mild. The deformity may progress despite orthotics.

Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Adult acquired flatfoot deformity (AAFD) is a painful condition resulting from the collapse of the longitudinal (lengthwise) arch of the foot. As the name suggests, this condition is not present at birth or during childhood. It occurs after the skeleton is fully matured. In the past it was referred to a posterior tibial tendon dysfunction (or insufficiency). But the name was changed because the condition really describes a wide range of flatfoot deformities. AAFD is most often seen in women between the ages of 40 and 60. This guide will help you understand how the problem develops, how doctors diagnose the condition, what treatment options are available.
Causes
Damage to the posterior tendon from overuse is the most common cause for adult acquired flatfoot. Running, walking, hiking, and climbing stairs are activities that add stress to this tendon, and this overuse can lead to damage. Obesity, previous ankle surgery or trauma, diabetes (Charcot foot), and rheumatoid arthritis are other common risk factors.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle. Symptoms, which may occur in some persons with flexible flatfoot, include. Pain in the heel, arch, ankle, or along the outside of the foot. ?Turned-in? ankle. Pain associated with a shin splint. General weakness / fatigue in the foot or leg.
Diagnosis
There are four stages of adult-acquired flatfoot deformity (AAFD). The severity of the deformity determines your stage. For example, Stage I means there is a flatfoot position but without deformity. Pain and swelling from tendinitis is common in this stage. Stage II there is a change in the foot alignment. This means a deformity is starting to develop. The physician can still move the bones back into place manually (passively). Stage III adult-acquired flatfoot deformity (AAFD) tells us there is a fixed deformity. This means the ankle is stiff or rigid and doesn???t move beyond a neutral (midline) position. Stage IV is characterized by deformity in the foot and the ankle. The deformity may be flexible or fixed. The joints often show signs of degenerative joint disease (arthritis).
Non surgical Treatment
Initial treatment consists of supporting the medial longitudinal arch (running the length of the foot) to relieve strain on the medial soft tissues. The most effective way to relieve pain on the tendon is to use a boot or brace, and once tenderness and pain has resolved, an orthotic device. A boot, brace, or orthotic has not been shown to correct or even prevent the progression of deformity. Orthotics can alleviate symptoms and may slow the progression of deformity, particularly if mild. The deformity may progress despite orthotics.
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
What Could You Do About Achilles Tendinitis Pains ?
Overview
 Achilles tendinitis is a common condition that causes pain along the back of the leg near the heel. The Achilles tendon is the largest tendon in the body. It connects your calf muscles to your heel bone and is used when you walk, run, and jump. Although the Achilles tendon can withstand great stresses from running and jumping, it is also prone to tendonitis, a condition associated with overuse and degeneration. Tendons become inflamed for a variety of reasons, and the action of pulling the muscle becomes irritating. If the normal, smooth gliding motion of the tendon is impaired, the tendon will become inflamed and movement will become painful. This is called tendonitis, meaning inflammation of the tendon. Achilles tendonitis is typically not related to a specific injury. The problem results from repetitive stress to the tendon. This often happens when we push our bodies to do too much, too soon, but other factors can make it more likely to develop tendinitis, including: a sudden increase in the amount or intensity of exercise activity, tight calf muscles, or a bone spur that has developed where the tendon attaches to the heel bone.
Achilles tendinitis is a common condition that causes pain along the back of the leg near the heel. The Achilles tendon is the largest tendon in the body. It connects your calf muscles to your heel bone and is used when you walk, run, and jump. Although the Achilles tendon can withstand great stresses from running and jumping, it is also prone to tendonitis, a condition associated with overuse and degeneration. Tendons become inflamed for a variety of reasons, and the action of pulling the muscle becomes irritating. If the normal, smooth gliding motion of the tendon is impaired, the tendon will become inflamed and movement will become painful. This is called tendonitis, meaning inflammation of the tendon. Achilles tendonitis is typically not related to a specific injury. The problem results from repetitive stress to the tendon. This often happens when we push our bodies to do too much, too soon, but other factors can make it more likely to develop tendinitis, including: a sudden increase in the amount or intensity of exercise activity, tight calf muscles, or a bone spur that has developed where the tendon attaches to the heel bone.
Causes
There are hundreds of tendons scattered throughout our body, but it tends to be a small handful of specific tendons that cause problems. These tendons usually have an area of poor blood supply that leads to tissue damage and poor healing response. This area of a tendon that is prone to injury is called a "watershed zone," an area when the blood supply to the tendon is weakest. In these watershed zones, they body has a hard time delivering oxygen and nutrients necessary for tendon healing, that's why we see common tendon problems in the same parts of the body. Tendonitis is most often an overuse injury. Often people begin a new activity or exercise that causes the tendon to become irritated. Tendon problems are most common in the 40-60 year old age range. Tendons are not as elastic and forgiving as in younger individuals, yet bodies are still exerting with the same force. Occasionally, there is an anatomical cause for tendonitis. If the tendon does not have a smooth path to glide along, it will be more likely to become irritated and inflamed. In these unusual situations, surgical treatment may be necessary to realign the tendon.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
In diagnosing Achilles tendonitis or tendonosis, the surgeon will examine the patient?s foot and ankle and evaluate the range of motion and condition of the tendon. The extent of the condition can be further assessed with x-rays or other imaging modalities.
Nonsurgical Treatment
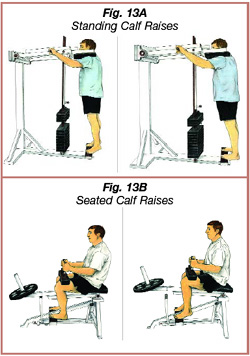
Treating Achilles tendinitis rarely requires much professional intervention. Ease the pain with OTC pain killers. Stretch and strengthen the Achilles tendon. Stop the condition from happening again. Doctors treating Achilles tendinitis will recommend the following options for accomplishing this. Pain Killers - Generally ibuprofen (Advil) or naproxen (Aleve) will ease the mild pain. Physical Therapy, Stretches and exercises devised to lengthen and strengthen the Achilles tendon will help reduce pain and prevent future recurrence. Orthopedic Supports, Heel-elevating insoles or other orthotic devices can reduce the strain on the Achilles tendon, helping ease the inflammation and pain.
Surgical Treatment
Surgical treatment for tendons that fail to respond to conservative treatment can involve several procedures, all of which are designed to irritate the tendon and initiate a chemically mediated healing response. These procedures range from more simple procedures such as percutaneous tenotomy61 to open procedures and removal of tendon pathology. Percutaneous tenotomy resulted in 75% of patients reporting good or excellent results after 18 months. Open surgery for Achilles tendinopathy has shown that the outcomes are better for those tendons without a focal lesion compared with those with a focal area of tendinopathy.62 At 7 months after surgery, 67% had returned to physical activity, 88% from the no-lesion group and 50% from the group with a focal lesion.
Prevention
You can take measures to reduce your risk of developing Achilles Tendinitis. This includes, Increasing your activity level gradually, choosing your shoes carefully, daily stretching and doing exercises to strengthen your calf muscles. As well, applying a small amount ZAX?s Original Heelspur Cream onto your Achilles tendon before and after exercise.
Achilles tendinitis is a common condition that causes pain along the back of the leg near the heel. The Achilles tendon is the largest tendon in the body. It connects your calf muscles to your heel bone and is used when you walk, run, and jump. Although the Achilles tendon can withstand great stresses from running and jumping, it is also prone to tendonitis, a condition associated with overuse and degeneration. Tendons become inflamed for a variety of reasons, and the action of pulling the muscle becomes irritating. If the normal, smooth gliding motion of the tendon is impaired, the tendon will become inflamed and movement will become painful. This is called tendonitis, meaning inflammation of the tendon. Achilles tendonitis is typically not related to a specific injury. The problem results from repetitive stress to the tendon. This often happens when we push our bodies to do too much, too soon, but other factors can make it more likely to develop tendinitis, including: a sudden increase in the amount or intensity of exercise activity, tight calf muscles, or a bone spur that has developed where the tendon attaches to the heel bone.
Causes
There are hundreds of tendons scattered throughout our body, but it tends to be a small handful of specific tendons that cause problems. These tendons usually have an area of poor blood supply that leads to tissue damage and poor healing response. This area of a tendon that is prone to injury is called a "watershed zone," an area when the blood supply to the tendon is weakest. In these watershed zones, they body has a hard time delivering oxygen and nutrients necessary for tendon healing, that's why we see common tendon problems in the same parts of the body. Tendonitis is most often an overuse injury. Often people begin a new activity or exercise that causes the tendon to become irritated. Tendon problems are most common in the 40-60 year old age range. Tendons are not as elastic and forgiving as in younger individuals, yet bodies are still exerting with the same force. Occasionally, there is an anatomical cause for tendonitis. If the tendon does not have a smooth path to glide along, it will be more likely to become irritated and inflamed. In these unusual situations, surgical treatment may be necessary to realign the tendon.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
In diagnosing Achilles tendonitis or tendonosis, the surgeon will examine the patient?s foot and ankle and evaluate the range of motion and condition of the tendon. The extent of the condition can be further assessed with x-rays or other imaging modalities.
Nonsurgical Treatment
Treating Achilles tendinitis rarely requires much professional intervention. Ease the pain with OTC pain killers. Stretch and strengthen the Achilles tendon. Stop the condition from happening again. Doctors treating Achilles tendinitis will recommend the following options for accomplishing this. Pain Killers - Generally ibuprofen (Advil) or naproxen (Aleve) will ease the mild pain. Physical Therapy, Stretches and exercises devised to lengthen and strengthen the Achilles tendon will help reduce pain and prevent future recurrence. Orthopedic Supports, Heel-elevating insoles or other orthotic devices can reduce the strain on the Achilles tendon, helping ease the inflammation and pain.
Surgical Treatment
Surgical treatment for tendons that fail to respond to conservative treatment can involve several procedures, all of which are designed to irritate the tendon and initiate a chemically mediated healing response. These procedures range from more simple procedures such as percutaneous tenotomy61 to open procedures and removal of tendon pathology. Percutaneous tenotomy resulted in 75% of patients reporting good or excellent results after 18 months. Open surgery for Achilles tendinopathy has shown that the outcomes are better for those tendons without a focal lesion compared with those with a focal area of tendinopathy.62 At 7 months after surgery, 67% had returned to physical activity, 88% from the no-lesion group and 50% from the group with a focal lesion.
Prevention
You can take measures to reduce your risk of developing Achilles Tendinitis. This includes, Increasing your activity level gradually, choosing your shoes carefully, daily stretching and doing exercises to strengthen your calf muscles. As well, applying a small amount ZAX?s Original Heelspur Cream onto your Achilles tendon before and after exercise.
What Is Plantar Fasciitis And Techniques To Get Rid Of It

Overview
The plantar fascia is a thick, ligamentous connective tissue that runs from the heel bone to the ball of the foot. This strong and tight tissue helps maintain the arch of the foot. It is also one of the major transmitters of weight across the foot as you walk or run. Thus, tremendous stress is placed on the plantar fascia, often leading to plantar fasciitis- a stabbing or burning pain in the heel or arch of the foot. Plantar fasciitis is particularly common in runners. People who are overweight, women who are pregnant and those who wear shoes with inadequate support are also at a higher risk. Prolonged plantar fasciitis frequently leads to heel spurs, a hook of bone that can form on the heel bone. The heel spur itself is not thought to be the primary cause of pain, rather inflammation and irritation of the plantar fascia is the primary problem.
Causes
The most frequent cause is an abnormal motion of the foot called excessive pronation. Normally, while walking or during long distance running, your foot will strike the ground on the heel, then roll forward toward your toes and inward to the arch. Your arch should only dip slightly during this motion. If it lowers too much, you have what is known as excessive pronation. For more details on pronation, please see the section on biomechanics and gait. Clinically not only those with low arches, but those with high arches can sometimes have plantar fasciitis. The mechanical structure of your feet and the manner in which the different segments of your feet are linked together and joined with your legs has a major impact on their function and on the development of mechanically caused problems. Merely having "flat feet" won't take the spring out of your step, but having badly functioning feet with poor bone alignment will adversely affect the muscles, ligaments, and tendons and can create a variety of aches and pains. Excess pronation can cause the arch of your foot to stretch excessively with each step. It can also cause too much motion in segments of the foot that should be stable as you are walking or running. This "hypermobility" may cause other bones to shift and cause other mechanically induced problems.
Symptoms
Plantar fasciitis generally occurs in one foot. Bilateral plantar fasciitis is unusual and tends to be the result of a systemic arthritic condition that is exceptionally rare among athletes. Males suffer from a somewhat greater incidence of plantar fasciitis than females, perhaps as a result of greater weight coupled with greater speed and ground impact, as well as less flexibility in the foot. Typically, the sufferer of plantar fasciitis experiences pain upon rising after sleep, particularly the first step out of bed. Such pain is tightly localized at the bony landmark on the anterior medial tubercle of the calcaneus. In some cases, pain may prevent the athlete from walking in a normal heel-toe gait, causing an irregular walk as means of compensation. Less common areas of pain include the forefoot, Achilles tendon, or subtalar joint. After a brief period of walking, the pain usually subsides, but returns again either with vigorous activity or prolonged standing or walking. On the field, an altered gait or abnormal stride pattern, along with pain during running or jumping activities are tell-tale signs of plantar fasciitis and should be given prompt attention. Further indications of the injury include poor dorsiflexion (lifting the forefoot off the ground) due to a shortened gastroc complex, (muscles of the calf). Crouching in a full squat position with the sole of the foot flat on the ground can be used as a test, as pain will preclude it for the athlete suffering from plantar fasciitis, causing an elevation of the heel due to tension in the gastroc complex.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
In general, plantar fasciitis is a self-limiting condition. Unfortunately, the time until resolution is often six to 18 months, which can lead to frustration for patients and physicians. Rest was cited by 25 percent of patients with plantar fasciitis in one study as the treatment that worked best. Athletes, active adults and persons whose occupations require lots of walking may not be compliant if instructed to stop all activity. Many sports medicine physicians have found that outlining a plan of “relative rest” that substitutes alternative forms of activity for activities that aggravate the symptoms will increase the chance of compliance with the treatment plan. It is equally important to correct the problems that place individuals at risk for plantar fasciitis, such as increased amount of weight-bearing activity, increased intensity of activity, hard walking/running surfaces and worn shoes. Early recognition and treatment usually lead to a shorter course of treatment as well as increased probability of success with conservative treatment measures.

Surgical Treatment
Surgery is considered only after 12 months of aggressive nonsurgical treatment. Gastrocnemius recession. This is a surgical lengthening of the calf (gastrocnemius) muscles. Because tight calf muscles place increased stress on the plantar fascia, this procedure is useful for patients who still have difficulty flexing their feet, despite a year of calf stretches. In gastrocnemius recession, one of the two muscles that make up the calf is lengthened to increase the motion of the ankle. The procedure can be performed with a traditional, open incision or with a smaller incision and an endoscope, an instrument that contains a small camera. Your doctor will discuss the procedure that best meets your needs. Complication rates for gastrocnemius recession are low, but can include nerve damage. Plantar fascia release. If you have a normal range of ankle motion and continued heel pain, your doctor may recommend a partial release procedure. During surgery, the plantar fascia ligament is partially cut to relieve tension in the tissue. If you have a large bone spur, it will be removed, as well. Although the surgery can be performed endoscopically, it is more difficult than with an open incision. In addition, endoscopy has a higher risk of nerve damage.
Prevention
More than with most sports injuries, a little bit of prevention can go a long way toward keeping you free from plantar fasciitis. Here are some tips to follow. Wear supportive shoes that fit you well. When your shoes start to show wear and can no longer give your feet the support they need, it's time to get a new pair. Runners should stop using their old shoes after about 500 miles of use. Have a trained professional at a specialty running store help you find the right pair for your foot type, and then keep your shoes tied and snug when you wear them. Stay in good shape. By keeping your weight in check, you'll reduce the amount of stress on your feet. Stretch your calves and feet before you exercise or play a sport. Ask an athletic trainer or sports medicine specialist to show you some dynamic stretching exercises. Start any new activity or exercise slowly and increase the duration and intensity of the activity gradually. Don't go out and try to run 10 miles the first time you go for a jog. Build up to that level of exercise gradually. Talk to your doctor about getting heel pads, custom shoe inserts, or orthotics to put in your shoes. Foot supports can help cushion your feet and distribute your weight more evenly. This is especially true for people with high arches or flat feet. Your doctor will be able to tell you if shoe inserts and supports might lower your chances of heel injury.
What Is Heel Discomfort

Overview
Your plantar fascia ligament helps the bones of your foot absorb gait-related shock. It also holds your toes firmly on the ground as your body passes over your foot. Plantar fasciosis can manifest in people who possess either flat feet or feet with high arches, and it most commonly causes pain or discomfort at the point where your plantar fascia attaches to your calcaneus, or heel bone. Plantar fasciosis, sometimes known as calcaneal spur syndrome or calcaneal enthesopathy, can involve stretching, tearing, and degeneration of your plantar fascia at its attachment site. In some cases, heel pain at this attachment site may be caused by other health problems, including certain types of arthritis. Your physician may run several tests to help determine the true cause of your plantar fascia pain and the most effective treatment methods to resolve your complaint.
Causes
The plantar fascia is designed to absorb the high stresses and strains we place on our feet. But, sometimes, too much pressure damages or tears the tissues. The body's natural response to injury is inflammation, which results in the heel pain and stiffness of plantar fasciitis.
Symptoms
Symptoms of plantar fasciitis can occur suddenly or gradually. When they occur suddenly, there is usually intense heel pain on taking the first morning steps, known as first-step pain. This heel pain will often subside as you begin to walk around, but it may return in the late afternoon or evening. When symptoms occur gradually, a more long-lasting form of heel pain will cause you to shorten your stride while running or walking. You also may shift your weight toward the front of the foot, away from the heel.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
More than 90% of patients with plantar fasciitis will improve within 10 months of starting simple treatment methods. Rest. Decreasing or even stopping the activities that make the pain worse is the first step in reducing the pain. You may need to stop athletic activities where your feet pound on hard surfaces (for example, running or step aerobics). Ice. Rolling your foot over a cold water bottle or ice for 20 minutes is effective. This can be done 3 to 4 times a day. Nonsteroidal anti-inflammatory medication. Drugs such as ibuprofen or naproxen reduce pain and inflammation. Using the medication for more than 1 month should be reviewed with your primary care doctor. Exercise. Plantar fasciitis is aggravated by tight muscles in your feet and calves. Stretching your calves and plantar fascia is the most effective way to relieve the pain that comes with this condition. Cortisone injections. Cortisone, a type of steroid, is a powerful anti-inflammatory medication. It can be injected into the plantar fascia to reduce inflammation and pain. Your doctor may limit your injections. Multiple steroid injections can cause the plantar fascia to rupture (tear), which can lead to a flat foot and chronic pain. Soft heel pads can provide extra support. Supportive shoes and orthotics. Shoes with thick soles and extra cushioning can reduce pain with standing and walking. As you step and your heel strikes the ground, a significant amount of tension is placed on the fascia, which causes microtrauma (tiny tears in the tissue). A cushioned shoe or insert reduces this tension and the microtrauma that occurs with every step. Soft silicone heel pads are inexpensive and work by elevating and cushioning your heel. Pre-made or custom orthotics (shoe inserts) are also helpful. Night splints. Most people sleep with their feet pointed down. This relaxes the plantar fascia and is one of the reasons for morning heel pain. A night splint stretches the plantar fascia while you sleep. Although it can be difficult to sleep with, a night splint is very effective and does not have to be used once the pain is gone. Physical therapy. Your doctor may suggest that you work with a physical therapist on an exercise program that focuses on stretching your calf muscles and plantar fascia. In addition to exercises like the ones mentioned above, a physical therapy program may involve specialized ice treatments, massage, and medication to decrease inflammation around the plantar fascia. Extracorporeal shockwave therapy (ESWT). During this procedure, high-energy shockwave impulses stimulate the healing process in damaged plantar fascia tissue. ESWT has not shown consistent results and, therefore, is not commonly performed. ESWT is noninvasive-it does not require a surgical incision. Because of the minimal risk involved, ESWT is sometimes tried before surgery is considered.

Surgical Treatment
In very rare cases plantar fascia surgery is suggested, as a last resort. In this case the surgeon makes an incision into the ligament, partially cutting the plantar fascia to release it. If a heel spur is present, the surgeon will remove it. Plantar Fasciitis surgery should always be considered the last resort when all the conventional treatment methods have failed to succeed. Endoscopic plantar fasciotomy (EPF) is a form of surgery whereby two incisions are made around the heel and the ligament is being detached from the heel bone allowing the new ligament to develop in the same place. In some cases the surgeon may decide to remove the heel spur itself, if present. Just like any type of surgery, Plantar Fascia surgery comes with certain risks and side effects. For example, the arch of the foot may drop and become weak. Wearing an arch support after surgery is therefore recommended. Heel spur surgeries may also do some damage to veins and arteries of your foot that allow blood supply in the area. This will increase the time of recovery.
Prevention
Do not walk barefoot on hard ground, particularly while on holiday. Many cases of heel pain occur when a person protects their feet for 50 weeks of the year and then suddenly walks barefoot while on holiday. Their feet are not accustomed to the extra pressure, which causes heel pain. If you do a physical activity, such as running or another form of exercise that places additional strain on your feet, you should replace your sports shoes regularly. Most experts recommend that sports shoes should be replaced after you have done about 500 miles in them.
What Exactly Triggers Plantar Fasciitis

Overview
Plantar Fasciitis is the Latin term for "inflammation of the plantar fascia". The plantar fascia is a thick, fibrous ligament that runs under the foot from the heel bone to the toes. It forms the arch of the foot and functions as our natural shock-absorbing mechanism. Unlike muscle tissue, the plantar fascia is not very elastic and therefore is very limited in its capacity to stretch or elongate. Herein lies the problem, when too much traction is placed on the plantar fascia (for various reasons) micro-tearing will occur, resulting in irritation, inflammation and pain. Plantar Fasciitis usually causes pain under the heel. However some people may experience pain under the arch of the foot. Both heel pain and arch discomfort are related to Plantar Fasciitis, with heel pain being far more common than arch pain.
Causes
Plantar Fasciitis is simply caused by overstretching of the plantar fascia ligament under the foot. So why is the ligament being overstretched? There are different factors, over-use, too much sports, running, walking or standing for long periods (e.g. because of your job) weight gain, our feet are designed to carry a 'normal' weight. Any excess weight places great pressure on the bones, nerves, muscles and ligaments in the feet, which sooner or later will have consequences. Even pregnancy (in the last 10 weeks) can cause foot problems! age, as we get older ligaments become tighter & shorter and msucles become weaker; the ideal circumstances for foot problems, unsupportive footwear, 'floppy' shoes with no support as well as thongs affect our walking pattern, walking barefoot, especially on hard surfaces like concrete or tiles, low arch and flat feet or over-pronation. An important contributing factor to Plantar Fasciitis is 'excess pronation' (or over-pronation). This is a condition whereby the feet roll over, the arches collapse and the foot elongates. This unnatural elongation puts excess strain on the ligaments, muscles and nerves in the foot. When the foot is not properly aligned, the bones unlock and cause the foot to roll inward. With every step taken your foot pronates and elongates, stretching the plantar fascia and causing inflammation and pain at the attachment of the plantar fascia into the heel bone. Re-alignment of the foot should therefore an important part of the treament regime.
Symptoms
Patients with plantar fasciitis typically experience pain underneath the heel and along the inner sole of the foot. In less severe cases, patients may only experience an ache or stiffness in the plantar fascia or heel that increases with rest (typically at night or first thing in the morning) following activities which place stress on the plantar fascia. These activities typically include standing, walking or running excessively (especially up hills, on uneven surfaces or in poor footwear such as thongs), jumping, hopping and general weight bearing activity. The pain associated with this condition may also warm up with activity in the initial stages of injury. As the condition progresses, patients may experience symptoms that increase during sport or activity, affecting performance. In severe cases, patients may walk with a limp or be unable to weight bear on the affected leg. Patients with this condition may also experience swelling, tenderness on firmly touching the plantar fascia (often on a specific spot on the inner aspect of the heel) and sometimes pain on performing a plantar fascia stretch.
Diagnosis
A physical exam performed in the office along with the diagnostic studies as an x-ray. An MRI may also be required to rule out a stress fracture, or a tear of the plantar fascia. These are conditions that do not normally respond to common plantar fasciitis treatment.
Non Surgical Treatment
Usually, the pain will ease in time. 'Fascia' tissue, like 'ligament' tissue, heals quite slowly. It may take several months or more to go. However, the following treatments may help to speed recovery. A combination of different treatments may help. Collectively, these initial treatments are known as 'conservative' treatments for plantar fasciitis. Rest your foot. This should be done as much as possible. Avoid running, excess walking or standing, and undue stretching of your sole. Gentle walking and exercises described below are fine. Footwear. Do not walk barefoot on hard surfaces. Choose shoes with cushioned heels and a good arch support. A laced sports shoe rather than an open sandal is probably best. Avoid old or worn shoes that may not give a good cushion to your heel. Heel pads and arch supports. You can buy various pads and shoe inserts to cushion the heel and support the arch of your foot. These work best if you put them in your shoes at all times. The aim is to raise your heel by about 1 cm. If your heel is tender, cut a small hole in the heel pad at the site of the tender spot. This means that the tender part of your heel will not touch anything inside your shoe. Place the inserts/pads in both shoes, even if you only have pain in one foot. Pain relief. Painkillers such as paracetamol will often ease the pain. Sometimes anti-inflammatory medicines such as ibuprofen are useful. These are painkillers but also reduce inflammation and may work better than ordinary painkillers. Some people find that rubbing a cream or gel that contains an anti-inflammatory medicine on to their heel is helpful. An ice pack (such as a bag of frozen peas wrapped in a tea towel) held to your foot for 15-20 minutes may also help to relieve pain. Exercises. Regular, gentle stretching of your Achilles tendon and plantar fascia may help to ease your symptoms. This is because most people with plantar fasciitis have a slight tightness of their Achilles tendon. If this is the case, it tends to pull at the back of your heel and has a knock-on effect of keeping your plantar fascia tight. Also, when you are asleep overnight, your plantar fascia tends to tighten up (which is why it is usually most painful first thing in the morning). The aim of these exercises is to loosen up the tendons and fascia gently above and below your heel. Your doctor may refer you to a physiotherapist for exercise guidance.

Surgical Treatment
When more-conservative measures aren't working, your doctor might recommend steroid shots. Injecting a type of steroid medication into the tender area can provide temporary pain relief. Multiple injections aren't recommended because they can weaken your plantar fascia and possibly cause it to rupture, as well as shrink the fat pad covering your heel bone. Extracorporeal shock wave therapy. In this procedure, sound waves are directed at the area of heel pain to stimulate healing. It's usually used for chronic plantar fasciitis that hasn't responded to more-conservative treatments. This procedure may cause bruises, swelling, pain, numbness or tingling and has not been shown to be consistently effective. Surgery. Few people need surgery to detach the plantar fascia from the heel bone. It's generally an option only when the pain is severe and all else fails. Side effects include a weakening of the arch in your foot.
Prevention
More than with most sports injuries, a little bit of prevention can go a long way toward keeping you free from plantar fasciitis. Here are some tips to follow. Wear supportive shoes that fit you well. When your shoes start to show wear and can no longer give your feet the support they need, it's time to get a new pair. Runners should stop using their old shoes after about 500 miles of use. Have a trained professional at a specialty running store help you find the right pair for your foot type, and then keep your shoes tied and snug when you wear them. Stay in good shape. By keeping your weight in check, you'll reduce the amount of stress on your feet. Stretch your calves and feet before you exercise or play a sport. Ask an athletic trainer or sports medicine specialist to show you some dynamic stretching exercises. Start any new activity or exercise slowly and increase the duration and intensity of the activity gradually. Don't go out and try to run 10 miles the first time you go for a jog. Build up to that level of exercise gradually. Talk to your doctor about getting heel pads, custom shoe inserts, or orthotics to put in your shoes. Foot supports can help cushion your feet and distribute your weight more evenly. This is especially true for people with high arches or flat feet. Your doctor will be able to tell you if shoe inserts and supports might lower your chances of heel injury.